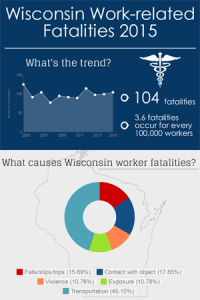
 According to the Bureau of Labor Statistics’ Census of Fatal Occupational Injuries, there were 104 Wisconsin workers who died due to injury in 2015. This number reflects an increase from 99 fatalities in 2014. Wisconsin’s overall fatality rate also increased from 3.5 to 3.6 deaths per 100,000. The number of workplace deaths in Wisconsin the past decade (2006-2015) range from 77 in 2008 to 114 in 2012, and average 98 fatalities annually.
According to the Bureau of Labor Statistics’ Census of Fatal Occupational Injuries, there were 104 Wisconsin workers who died due to injury in 2015. This number reflects an increase from 99 fatalities in 2014. Wisconsin’s overall fatality rate also increased from 3.5 to 3.6 deaths per 100,000. The number of workplace deaths in Wisconsin the past decade (2006-2015) range from 77 in 2008 to 114 in 2012, and average 98 fatalities annually.
The final count of occupational fatalities in the U.S. in 2015 was 4,836, according to national figures released last Friday. This was an increase from the revised total of 4,821 in 2014. The overall fatality rate decreased from 3.43 to 3.38 cases per 100,000 full time employees.
Key findings for Wisconsin in 2015:
- Work-related fatality rates decreased for agriculture, professional business services, and education and health services industries, and increased for construction, transportation, manufacturing, and wholesale and retail trade.
- Transportation incidents caused the most fatalities, a 21% increase from the prior year.
- Exposures to harmful substances or environments increased from 5 to 11 incidents.
- Fatal injuries to females in 2015 decreased from 12 in 2014 to 4 in 2015.
- Employees age 55 to 64 sustained the highest number of fatalities.
Industry
In 2015, 95 of the 104 work-related deaths in Wisconsin occurred within private industry. Public sector worker deaths increased from 5 deaths in 2014 to 9 in 2015. Agriculture, fishing, forestry, and hunting
fatality count decreased from 27 to 26. Fatalities in the professional and business services industry decreased from 13 to 7, while the trade, transportation, and utilities increased from 17 to 24. Manufacturing industry deaths rose from 11 in 2014 to 14 in 2015, while fatalities in the construction industry remained unchanged at 14.
Event
Transportation incidents comprised the highest number of fatal work injuries with 46 incidents, an increase from 39 incidents in 2014. Falls, slips, and trips increased slightly from 16 in 2014 to 17 last year, while fatal contact injuries decreased from 22 to 18. Violent events decreased from 15 in 2014 to 11 in 2015. Deaths due to exposure to harmful substance or environments increased from 5 to 11 incidents.
Worker Characteristics and Occupation
Of the 104 fatalities, 14 workers were in contractor status, and 39 were self-employed. The highest number of fatal work injuries occurred among age group 55 to 64 with 26 deaths, followed by age 45 to 54 with 22, and age 65 years or older with 19. Management occupations sustained the greatest number of fatal injuries in 2015 at 20 incidents, followed by transportation and material moving occupations with 19 deaths. Construction and extraction occupations sustained 13 fatalities, 11 deaths occurred among production workers and 10 among farming, fishing, and forestry occupations.
Background of Census of Fatal Occupational Injuries
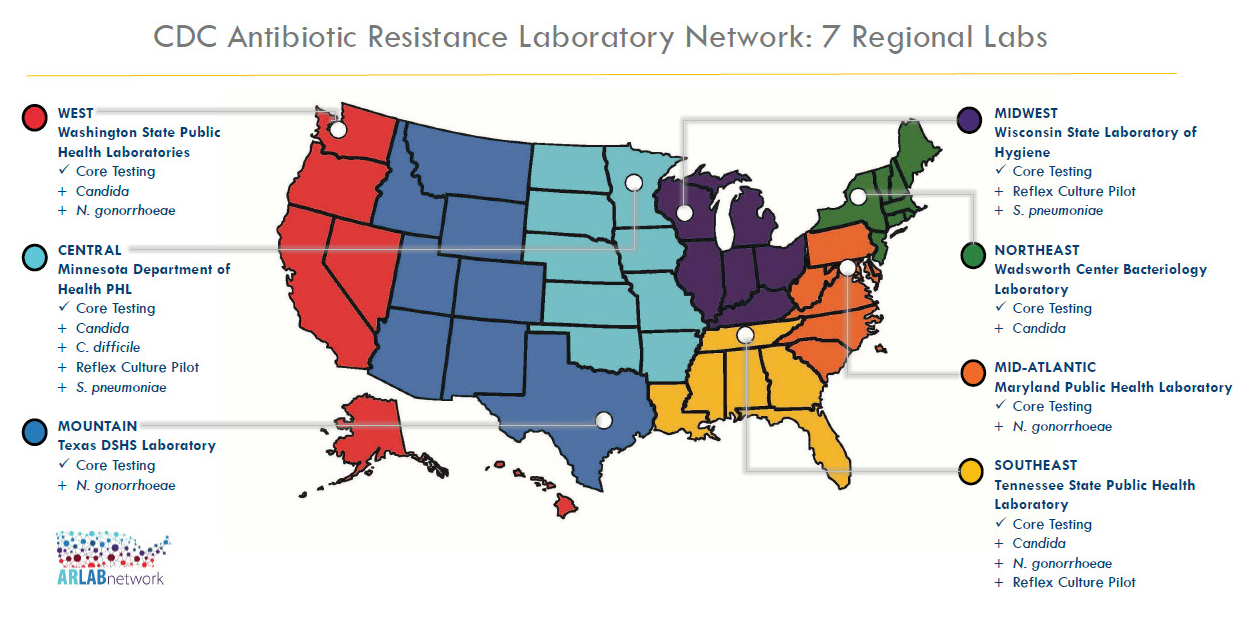
The Census of Fatal Occupational Injuries, part of the BLS occupational safety and health statistics program, compiles a count of all fatal work injuries occurring in the United States during the calendar year. The program uses diverse state, federal, and independent data sources to identify, verify, and describe fatal work injuries. The Wisconsin State Laboratory of Hygiene (WSLH), a part of the University of Wisconsin-Madison, is the state’s public, environmental and occupational health laboratory. The WSLH’s Bureau of Labor Statistics/Occupational Safety and Health Statistics Program has a cooperative agreement with the U.S. Bureau of Labor Statistics to conduct the Census of Fatal Occupational Injuries in Wisconsin.
For more about Wisconsin Work-related fatalities, go to www.slh.wisc.edu/bls.
For more about U.S. Work-related fatalities, go to https://www.bls.gov/iif/news.htm
 The situation is terrifying. A seemingly healthy person suddenly collapses – unconscious – and tragically dies from cardiac arrest. Family members in their grief ask “Why?” and maybe even “Can it happen to us too?”
The situation is terrifying. A seemingly healthy person suddenly collapses – unconscious – and tragically dies from cardiac arrest. Family members in their grief ask “Why?” and maybe even “Can it happen to us too?”
 According to estimates from the U.S. Bureau of Labor Statistics’ Survey of Occupational Injuries and Illnesses (SOII), there were 78,800 total injuries and illnesses reported by Wisconsin employers in 2015, which occurred at a rate of 3.6 cases per 100 equivalent full-time workers. This is a decline from 4.0 in 2013 and 2014. Nationwide, the total injury and illness case rate declined from 3.4 to 3.3 per 100 full-time workers.
According to estimates from the U.S. Bureau of Labor Statistics’ Survey of Occupational Injuries and Illnesses (SOII), there were 78,800 total injuries and illnesses reported by Wisconsin employers in 2015, which occurred at a rate of 3.6 cases per 100 equivalent full-time workers. This is a decline from 4.0 in 2013 and 2014. Nationwide, the total injury and illness case rate declined from 3.4 to 3.3 per 100 full-time workers. Did you know the
Did you know the